Newsletter August-September 2014
 Hello,
Hello,
Welcome to the latest newsletter. We hope you enjoy reading this edition. If you decide, once you’re on this page, you’d like to go to the main website instead just click on the logo above.
Here is the 3rd part (of 4) which looks at the general causes behind musculoskeletal pain.
Don’t forget we’re on Facebook and Twitter, we would be grateful if you’d follow the links at the bottom of the page (in the contacts section) to show your support.
Kind Regards,
James & Katy.
To recap from the last newsletter, a question that often get asked by clients is ‘how did this (injury/pain) suddenly happen?’. The answer is usually because of one of 4 reasons:
1. Overuse / Overtraining
2. Poor posture
3. Trauma
4. A medical condition
In fact, all 4 can be inter-related as the reason, it may not be just one alone. For example, a medical condition (such as arthritis) could cause pain and swelling in itself, but could also lead to poor posture, which in turn could lead to overuse, or overtraining of structures elsewhere in the body.
Extrapolating this idea, you could easily substitute a medical condition, for a trauma (such as a strain, or sprain). The injury itself can create it’s own pain, swelling etc. but then during the healing process your posture and movement could change (a limp for example) leading to poor posture and so on. In this newsletter we’ll look specifically at No.3 on the list above; trauma.
3. Trauma
Both physical and mental trauma can be one of the most destructive things to happen to the body. The immediacy of physical trauma’s effect depends not only on the nature of the injury, but also any surgery required to repair it. Let’s look at a fairly common sporting injury; a complete tear of either the anterior cruciate (ACL) and / or the posterior cruciate ligament (PCL) in the knee. Firstly, to understand the seriousness of an injury such as this, it’s important to know what role ligaments play.
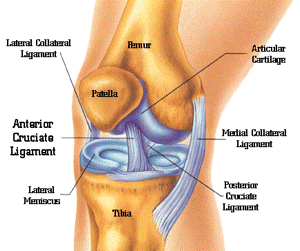
The function of a ligament is to provide stability to the joint and also restrict the range of movement to within safe limits. However, under extreme duress, or repeated lower level strain, it is possible to stretch, partially tear, or completely rupture a ligament.
The knock on effect of a complete tear is that the joint will lose a majority of it’s inherent stability and ‘safe’ range of movement. In terms of the knee the femur will now also shift either forwards, or backwards (depending on whether it was the ACL or the PCL that was ruptured).
The most common thing to do for a complete rupture would be to go for a surgical repair as soon as the swelling from the impact that caused the tear has subsided. However, even after surgery the knee will not be as strong as before, there will be scar tissue around the joint and it will more than likely require a reasonable amount of rehabilitation work. There’s also a fair chance your walking (gait) will have changed due to the pain and inflammation, and with it your posture will have altered as well. As we know from the last newsletter, poor posture is also a cause of muscle and joint pain, but in this instance they are now working in tandem. If these additional postural and mechanical changes are not looked at after the surgery, and you maintain a limp or awkward walking stride, then you can have secondary problems in the future (even though the knee itself has been repaired). These secondary problems could take the form of pain in the ankle, hip, low back, neck, or discomfort in the opposite leg.